

Women’s Orthopedic & Pelvic Physical Therapy...

ME/CFS in Women: Why Fatigue, Pain, and Exercise Intolerance Require a Different Physical Therapy Approach
read more
Including male, female, pediatric, transgender and nonbinary chronic pelvic pain, urinary dysfunction such as incontinence, prostatitis, sexual dysfunction, pregnancy, back pain, upcoming events and more.

Women’s Orthopedic & Pelvic Physical Therapy...

At Fusion Wellness and Femina Physical Therapy...

Skid marks and fecal accidents can be a sign of...

Are You Experiencing Erectile Dysfunction Post...

This article explores how physical therapists...

Physical therapy for trans individuals is an...

Softwave low intensity shockwave therapy is a...

Pelvic floor pain can be a tricky thing for many...

Read on to find out more about Low Intensity...

Physical Therapy Can Play a Part in Effective...

When a Squatty Potty isn't Enough: How Pelvic...

Learn about low intensity shockwave therapy for...

Learn All About Childhood Bedwetting and...

An In Depth Look at Bladder Control for Your...

Best Exercise for Each Decade of Life: Exercises...

There is growing research for the role of pelvic...

Individuals affected by endometriosis often...

This month is Bladder Health awareness month and...

Want to start a spin class? Afraid of returning...
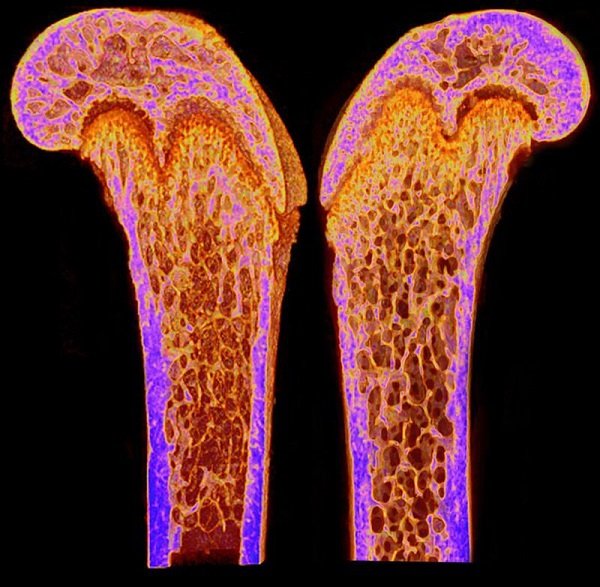
May is Osteoporosis Awareness Month. Did...

Building Your Own Post-run Recovery Routine A...

10 Strength, Conditioning, and Balance Exercises...

Road to Boston Marathon Part 1 A Tribute to the...

Male Dysorgasmia is on the Rise In our practice,...

Over 1 million people in the United States...

Restless Legs Syndrome (or RLS) Restless legs...
Restless Leg Syndrome (or RLS) Restless leg...

Causes & Treatments for Lower Urinary Tract...

Is There Really a Relationship Between Grip...

It has long been recognized in the Pelvic...
A Recent Pilot Study Looked at the Connection...

Overview: Urinary Incontinence About 13 million...

This article introduces common unwanted side...

This article will go over what a Tarlov cyst...

In this Blog Post We Highlight an Important...

Highlight on Mens Pelvic Pain June is Men's...

Scoliosis and the Pelvic Floor - A Primer Part 2...

An Overview of Functional Scoliosis and...

Studies Have Shown that Mindfulness Can Help...

Research draws a connection between histamines...

Bedwetting In Children - When is it a problem? I...

Frequent Urinary Tract Infections (UTIs) in...
Did you know that chronic pelvic pain can happen...

September is Healthy Aging Month - Learn...

A 2019 literature review by Twitchell et al....

As an approved way to get exercise during the...

Doctors have known for decades that smoking...

Are You Considering Pelvic Floor Therapy for...

Radical prostatectomy is a procedure that is...

When talking to some of my patients, I’ve...

I just returned to Los Angeles after completing...

Asking Yourself "Why do my testicles hurt?" Read...
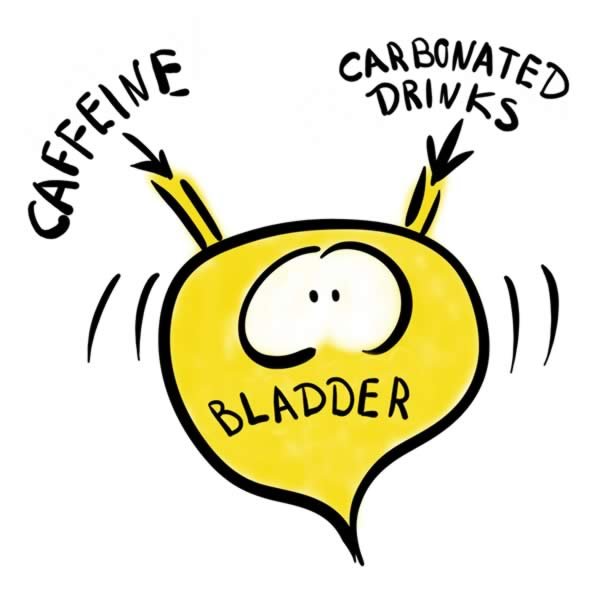
Did you know specific food and drinks can...

May is Pelvic Pain Awareness month and healthy...

Did you know that riding a bike that doesn’t fit...
How to prevent back pain for your child With the...

Childhood Constipation and how Pelvic Floor...

While occasional daytime and nighttime accidents...

Managing Prostatitis Related Pain is Possible...
Did You Know That You Can Practice Yoga Therapy...

Ways Prostatitis Related Pelvic Pain Can Be...

This article will review how prostatitis can...
Most people experience occassional constipation....
Pelvic floor physical therapy is one of the best...

In my last post, “Why You Should Be Doing Kegels...
I am proud to announce the official book release...

Wondering Why You Should be Doing Kegels? Read...
What are Kegels? Kegels are a contraction of a...

As an expert in the field of all facets of postpartum care, I believe that a measured approach to exercise is vitally important to achieve optimum pelvic health without complications, and Daniella so graciously states in the opening paragraph of her article:
When you visit our space on Amazon you will find a wide variety of products that will help in your quest to not just better pelvic health, but to your overall health and wellbeing too! Click anywhere in this ad to go there now and find what you need!

Whilst recovering in hospital after the birth of her first child, our founder Sinead O’Donovan decided that new mums deserved more help getting back to their busy lives. Drawing on her extensive medical and bio-mechanical background, Sinead envisaged a garment that would be comfortable for new mums to wear all day whilst giving her all the support she and her body need.

In Heather’s own words:
I thought it’s finally time to share one of my post-op recovery secrets — I’ve been loving that supported life in my @srchealth compression leggings since my hip labral repair surgery last October. When I wear them, my chronic left SI joint hurts less and my legs feel like they’re being micro-massaged all day long!
Click here to shop the full SRC Health line, and use code FEMINA at checkout for special pricing!
Whilst recovering in hospital after the birth of her first child, our founder Sinead O’Donovan decided that new mums deserved more help getting back to their busy lives. Drawing on her extensive medical and bio-mechanical background, Sinead envisaged a garment that would be comfortable for new mums to wear all day whilst giving her all the support she and her body need.

Click here and use code FEMINAPT to save $10 off your first $50 purchased.